Review ENBREL’s clinical study designs and results in treating patients with moderate to severe plaque psoriasis (PsO)
Recapture results after withdrawal and retreatment
The US Psoriasis Pivotal Trial was a two-part, multicenter, phase 3 study consisting of a 24-week double-blind period followed by a 60-week withdrawal and retreatment period. A total of 652 patients with active but clinically stable plaque psoriasis involving at least 10% of body surface area (BSA) and a minimum Psoriasis Area and Severity Index (PASI) score of 10. Patients were randomized to receive ENBREL 50 mg twice weekly (BIW, n=164), ENBREL 25 mg BIW (n=162), ENBREL 25 mg weekly (QW, n=160), or placebo (n=166) for 12 weeks. After Week 12, patients in the placebo group began blinded treatment with ENBREL 25 mg BIW.1,2
At Week 24, patients with 50% PASI improvement from baseline discontinued ENBREL treatment until disease relapse (loss of the 50% PASI improvement that was obtained by Week 24). Upon relapse, patients resumed blinded ENBREL therapy at the same dose they had received from Weeks 13 to 24.1
A post hoc analysis was conducted for an open-label extension (OLE), including 439 patients from the US Psoriasis Pivotal Trial after completing a minimum of 60 weeks in the primary study. Patients in the OLE received ENBREL 50 mg QW for the first 12 weeks followed by a dose escalation of 50 mg BIW for patients with an inadequate clinical response.3,4


| Age (mean) | 45 years |
| Male | 67% |
| Caucasian | 87% |
| Weight (mean) | 208 lb (86-437 lb) |
| Body mass index (mean) | 31 |
| BSA involvement (mean) | 29% |
| PsO duration (mean) | 19 years |
| PASI (mean) | 18 |


*Patients who completed 12 weeks of retreatment.1
†Only patients with ≥50% PASI improvement from baseline at Week 24 discontinued ENBREL treatment and were enrolled in this part of the study.1
‡Last observation carried forward (LOCF).
§As observed.
94% of the Week 24 response was recaptured at Week 607


–Patients (n=37) in the ENBREL 50 mg BIW group after Week 12 during the US Psoriasis Pivotal Trial who were randomized to the 50 mg QW group through 72 weeks of the OLE7
–Patients (n=284) who increased their ENBREL dose to 50 mg BIW after Week 12 during the OLE8
–Patients (n=75) in the ENBREL 50 mg QW continuous arm through 72 weeks who had >30 days off treatment between the US Psoriasis Pivotal Trial and the OLE9
–Patients (n=5) met 2 of these exclusion criteria: received ENBREL 50 mg BIW who had >30 days off treatment
sPGA, static Physician's Global Assessment.
12-week and 120-week results
The Global Psoriasis Pivotal Trial was a 48-week, multicenter, double-blind, randomized, phase 3 trial of 611 adult patients with active but clinically stable PsO involving at least 10% of BSA and a minimum PASI score of 10. 583 patients received at least one dose of study drug and these were the 583 patients included in the primary analysis. Patients were randomized to receive ENBREL 50 mg (n=194), ENBREL 25 mg (n=196), or placebo (n=193) BIW over 12 weeks. After Week 12, all patients (N=583) received open-label ENBREL 25 mg BIW over 36 weeks. Patients were limited to low- to moderate-strength topical corticosteroids in the axillary, groin, and scalp regions. A post hoc analysis was conducted for an OLE, including 473 patients from the Global Psoriasis Pivotal Trial after completing a minimum of 36 weeks of open-label treatment. Patients in the OLE received ENBREL 50 mg QW.4,10,11


| Age (median) | 45 years |
| Male | 66% |
| Caucasian | 91% |
| Weight (mean) | 194 lb |
| Body mass index (mean) | 30 |
| BSA involvement (mean) | 28% |
| PsO duration (mean) | 20 years |
| PASI (mean) | 19 |


–Patients who increased their ENBREL dose to 50 mg BIW after Week 12 during the OLE (n=307)8
–Patients in the ENBREL 50 mg QW continuous arm through 72 weeks who had >30 days of treatment between Global Psoriasis Pivotal Trial and the OLE9


ITT, intent-to-treat; LOCF, Last observation carried forward; mITT, modified intent-to-treat; NRI, nonresponder imputation; RCT, randomized controlled trial.
Patient-reported outcomes for pain and itch
The Phase 3 Study was a 12-week, randomized, double-blind, placebo-controlled, parallel-group study of 618 patients with active and clinically significant plaque psoriasis involving ≥10% BSA and a minimum PASI score of 10. Patients received ENBREL 50 mg BIW (n=311) or placebo BIW (n=307).16
*Subjects were asked to rate their skin pain and itch as a component of a psoriasis clinical trial, so it can be reasonably assumed that the subjects answered this question attributing the skin pain and itch to their moderate to severe plaque psoriasis.


58% improvement in mean itch score relative to the mean baseline score.17


68% improvement in mean skin pain score relative to the mean baseline score17


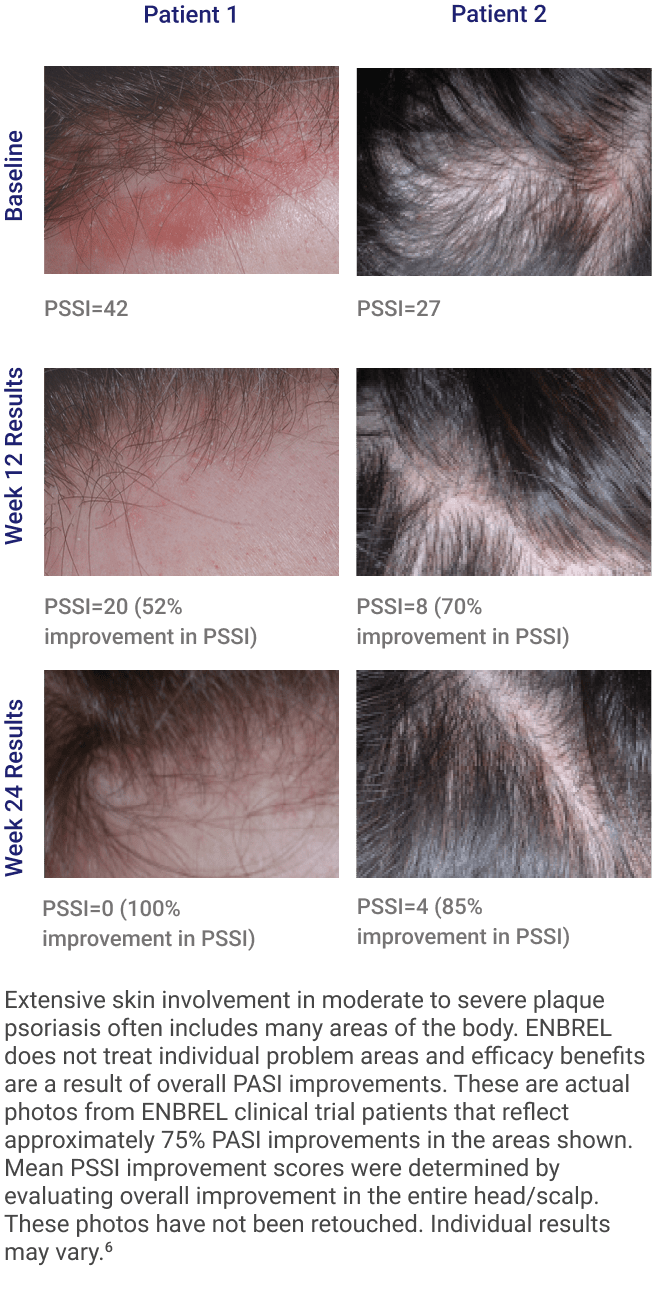
Psoriasis Scalp Severity Index (PSSI) results for patients with PsO scalp involvement
The ENBREL Scalp Involvement Study was a 24-week, multicenter, double-blind, randomized, placebo-controlled trial of 124 patients with active but clinically stable plaque PsO involving BSA ≥10%, a minimum PASI score of 10, ≥30% involvement of the scalp surface area (SSA), and a minimum PSSI score of 15. Patients received ENBREL 50 mg BIW (n=62) or placebo BIW (n=62) over 12 weeks. After Week 12, patients received ENBREL 50 mg QW (if initially randomized to ENBREL 50 mg BIW, n=58) or ENBREL 50 mg BIW (if initially randomized to placebo, n=54).18,19


*124 patients were randomized; 121 received at least one dose.
| Age (mean) | 42 years |
| Male | 56% |
| Caucasian | 73% |
| Weight (mean) | 197 lb (92-337 lb) |
| Body mass index (mean) | 31 |
| BSA involvement (mean) | 22% |
| Scalp improvement (mean) | 64% |
| PsO duration (mean) | 18 years |
| PASI (mean) | 18 |
| PSSI (mean) | 35 |


*ITT analysis with LOCF imputation.
†P<0.0001 vs placebo.
78% mean PASI improvement at Week 2419


*ITT analysis with LOCF imputation.

Patients experienced less scalp itch with ENBREL


*Subjects were asked to rate their scalp itch as a component of a psoriasis clinical trial, so it can be reasonably assumed that the subjects answered this question attributing the scalp itch to their moderate to severe plaque psoriasis.
†ITT analysis with LOCF imputation.
Patients experienced less scalp pain with ENBREL


*Subjects were asked to rate their scalp pain as a component of a psoriasis clinical trial, so it can be reasonably assumed that the subjects answered this question attributing the scalp pain to their moderate to severe plaque psoriasis.
†ITT analysis with LOCF imputation.

Evaluated patients with plaque PsO between 4 and 17 years of age over 48 weeks
The Pediatric Psoriasis Pivotal Study was a 48-week, randomized, double-blind, placebo-controlled US and Canadian study (parent study) in 211 patients with moderate to severe plaque PsO between 4 and 17 years of age. Patients were randomized in double-blind treatment to receive ENBREL once weekly (QW, dosing of 0.8 mg/kg up to a maximum dose of 50 mg, n=106) or placebo (n=105) over 12 weeks. After Week 12, all patients (N=208) received open-label ENBREL QW for 24 weeks. After Week 36, patients were re-randomized in double-blind treatment to receive ENBREL QW (n=69) or placebo (n=69) for 12 weeks. The primary study was followed up by a 264-week (5-year; N=182) OLE. All patients in the OLE received ENBREL QW.6,23,24


*If PASI score worsened >50% at or after Week 4, patients could receive open-label ENBREL.
†Patients who did not reach PASI 50 at Week 24 or PASI 75 at Week 36 could discontinue or add low to moderate topical corticosteroids.
‡Patients who lost PASI 75 resumed open-label ENBREL treatment.
§At Week 312, n=69.
| 4-17 years old |
Moderate to severe plaque PsO defined as:
|
| Disease duration ≥6 months |
| Had a history of receiving phototherapy or systemic therapy, or were inadequately controlled on topical therapy |
Age, mean
|
13 years 36% 64% |
| Weight, mean (range) | 136.3 lb (37.9-371.0 lb) |
| Height, mean (range) | 61.2 in (40.9-75.0 in) |
| BSA involvement, mean (range) | 25% (10.0-95.0) |
| Previously treated with systemic therapy or phototherapy | 57% |
| Male | 51% |
| Caucasian** | 75% |
| Duration of PsO, mean | 6.0 years |
| PASI, mean (range) | 18.5 (12.0-56.7) |
| PASI, median | 16.4 |
**25% were Black or African American, Hispanic or Latino, Asian, Native Hawaiian or Other Pacific Islander, or Other.27


*Open-label period or incomplete-responder arm; patients could enter the incomplete-responder arm at Week 24 or Week 36.
† ITT NRI analysis.
Results through 312 weeks in the combined primary study and open-label extension


*Patients were treated and evaluated for 5 years or until they turned 18, whichever came last. Seven patients discontinued due to disease progression (3.8%).29
Consider OLE study limitations when interpreting the above results. The OLE study is not blinded, not controlled, and includes inherent self-selection bias. A total of 6 patients (3.3%) had adverse events that led to discontinuation of ENBREL and 5 patients (2.7%) had adverse events that led to discontinuation of the study.28


*ENBREL: n=106 through Week 12 and n=105 through Week 36. Placebo/ENBREL: n=105 through Week 12 and n=103 through Week 36.
Results through 312 weeks in the combined primary study and open-label extension
*ITT NRI analysis.


Consider OLE study limitations when interpreting the above results. The OLE study is not blinded, not controlled, and includes inherent self-selection bias. A total of 6 patients (3.3%) had adverse events that led to discontinuation of ENBREL and 5 patients (2.7%) had adverse events that led to discontinuation of the study.28


*Healthy weight = body mass index (BMI) 5th-84th percentile; overweight = BMI 85th-94th percentile; obese = BMI ≥95th percentile.32
Prescription Enbrel® (etanercept) is administered by injection.
IMPORTANT SAFETY INFORMATION AND INDICATIONS
SERIOUS INFECTIONS
Patients treated with ENBREL are at increased risk for developing serious infections that may lead to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids or were predisposed to infection because of their underlying disease. ENBREL should not be initiated in the presence of sepsis, active infections, or allergy to ENBREL or its components. ENBREL should be discontinued if a patient develops a serious infection or sepsis. Reported infections include: 1) Active tuberculosis (TB), including reactivation of latent TB. Patients with TB have frequently presented with disseminated or extrapulmonary disease. Test patients for latent TB before ENBREL use and periodically during therapy. Initiate treatment for latent infection prior to ENBREL use, 2) Invasive fungal infections, including histoplasmosis, coccidioidomycosis, candidiasis, aspergillosis, blastomycosis, and pneumocystosis. Patients with histoplasmosis or other invasive fungal infections may present with disseminated, rather than localized, disease. Antigen and antibody testing for histoplasmosis may be negative in some patients with active infection. Consider empiric antifungal therapy in patients at risk for invasive fungal infections who develop severe systemic illness, and 3) Bacterial, viral, and other infections due to opportunistic pathogens, including Legionella and Listeria.
The risks and benefits of treatment with ENBREL should be carefully considered prior to initiating therapy in patients 1) with chronic or recurrent infection, 2) who have been exposed to TB, 3) who have resided or traveled in areas of endemic TB or endemic mycoses, or 4) with underlying conditions that may predispose them to infections such as advanced or poorly controlled diabetes. Monitor patients closely for the development of signs and symptoms of infection during and after treatment with ENBREL, including the possible development of TB in patients who tested negative for latent TB prior to initiating therapy.
MALIGNANCIES
Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with tumor necrosis factor (TNF) blockers, including ENBREL.
In adult clinical trials of all TNF blockers, more cases of lymphoma were seen compared to control patients. The risk of lymphoma may be up to several-fold higher in RA patients. The role of TNF blocker therapy in the development of malignancies is unknown.
Cases of acute and chronic leukemia have been reported in association with postmarketing TNF blocker use in RA and other indications. The risk of leukemia may be higher in patients with RA (approximately 2-fold) than the general population.
Melanoma and non-melanoma skin cancer (NMSC) have been reported in patients treated with TNF blockers, including ENBREL. Periodic skin examinations should be considered for all patients at increased risk for skin cancer.
Pediatric Patients
In patients who initiated therapy at ≤18 years of age, approximately half of the reported malignancies were lymphomas (Hodgkin's and non-Hodgkin's lymphoma). Other cases included rare malignancies usually associated with immunosuppression and malignancies that are not usually observed in children and adolescents. Most of the patients were receiving concomitant immunosuppressants.
NEUROLOGIC REACTIONS
Treatment with TNF-blocking agents, including ENBREL, has been associated with rare (<0.1%) cases of new onset or exacerbation of central nervous system demyelinating disorders, some presenting with mental status changes and some associated with permanent disability, and with peripheral nervous system demyelinating disorders. Cases of transverse myelitis, optic neuritis, multiple sclerosis, Guillain-Barré syndromes, other peripheral demyelinating neuropathies, and new onset or exacerbation of seizure disorders have been reported in postmarketing experience with ENBREL therapy. Prescribers should exercise caution in considering the use of ENBREL in patients with preexisting or recent-onset central or peripheral nervous system demyelinating disorders.
NEW ONSET OR WORSENING OF HEART FAILURE
Cases of worsening congestive heart failure (CHF) and, rarely, new-onset cases have been reported in patients taking ENBREL. Caution should be used when using ENBREL in patients with CHF. These patients should be carefully monitored.
HEMATOLOGIC REACTIONS
Rare cases of pancytopenia, including aplastic anemia, some fatal, have been reported. The causal relationship to ENBREL therapy remains unclear. Exercise caution when considering ENBREL in patients who have a previous history of significant hematologic abnormalities. Advise patients to seek immediate medical attention if they develop signs or symptoms of blood dyscrasias or infection. Consider discontinuing ENBREL if significant hematologic abnormalities are confirmed.
HEPATITIS B REACTIVATION
Reactivation of hepatitis B has been reported in patients who were previously infected with hepatitis B virus (HBV) and received concomitant TNF-blocking agents, including ENBREL. Most reports occurred in patients also taking immunosuppressive agents, which may contribute to hepatitis B reactivation. Exercise caution when considering ENBREL in these patients.
ALLERGIC REACTIONS
Allergic reactions associated with administration of ENBREL during clinical trials have been reported in <2% of patients. If an anaphylactic reaction or other serious allergic reaction occurs, discontinue administration of ENBREL and initiate appropriate therapy immediately.
IMMUNIZATIONS
Avoid concurrent administration of live vaccines with ENBREL. Patients, if possible, should be brought up to date with all immunizations prior to initiating ENBREL. In patients with exposure to varicella virus, temporarily discontinue ENBREL and consider prophylactic treatment with Varicella Zoster Immune Globulin.
AUTOIMMUNITY
Autoantibodies may develop with ENBREL, and rarely lupus-like syndrome or autoimmune hepatitis may occur. These may resolve upon withdrawal of ENBREL. Stop ENBREL if findings suggestive of lupus-like syndrome or autoimmune hepatitis develop and evaluate the patient.
NOT RECOMMENDED FOR GRANULOMATOSIS WITH POLYANGIITIS PATIENTS ON IMMUNOSUPPRESSANTS
The use of ENBREL in patients with granulomatosis with polyangiitis receiving immunosuppressive agents (eg, cyclophosphamide) is not recommended.
INCREASED MORTALITY IN PATIENTS WITH MODERATE TO SEVERE ALCOHOLIC HEPATITIS
Based on a study of patients treated for alcoholic hepatitis, exercise caution when using ENBREL in patients with moderate to severe alcoholic hepatitis.
ADVERSE REACTIONS
The most commonly reported adverse reactions in RA clinical trials were injection site reaction and infection. In clinical trials of all other adult indications, adverse reactions were similar to those reported in RA clinical trials.
In general, the adverse reactions in pediatric patients were similar in frequency and type as those seen in adult patients. The types of infections reported in pediatric patients were generally mild and consistent with those commonly seen in the general pediatric population.
DRUG INTERACTIONS
The use of ENBREL in patients receiving concurrent cyclophosphamide therapy is not recommended. The risk of serious infection may increase with concomitant use of abatacept therapy. Concurrent therapy with ENBREL and anakinra is not recommended. Hypoglycemia has been reported following initiation of ENBREL therapy in patients receiving medication for diabetes, necessitating a reduction in anti-diabetic medication in some of these patients.
Please see Prescribing Information and Medication Guide.
INDICATIONS
ENBREL is indicated for reducing signs and symptoms, inducing major clinical response, inhibiting the progression of structural damage, and improving physical function in patients with moderately to severely active rheumatoid arthritis. ENBREL can be initiated in combination with methotrexate (MTX) or used alone.
ENBREL is indicated for reducing signs and symptoms, inhibiting the progression of structural damage of active arthritis, and improving physical function in adult patients with psoriatic arthritis. ENBREL can be used with or without MTX.
ENBREL is indicated for the treatment of patients 4 years or older with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.
ENBREL is indicated for reducing signs and symptoms in patients with active ankylosing spondylitis.
ENBREL is indicated for reducing signs and symptoms of moderately to severely active polyarticular juvenile idiopathic arthritis in patients 2 years of age and older.
ENBREL is indicated for the treatment of active juvenile psoriatic arthritis in pediatric patients 2 years of age and older.
Prescription Enbrel® (etanercept) is administered by injection.
IMPORTANT SAFETY INFORMATION AND INDICATIONS
SERIOUS INFECTIONS
Patients treated with ENBREL are at increased risk for developing serious infections that may lead to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids or were predisposed to infection because of their underlying disease. ENBREL should not be initiated
Patients treated with ENBREL are at increased risk for developing serious infections that may lead to
References: