Review ENBREL's clinical study designs and results in treating patients with moderate to severe rheumatoid arthritis (RA)
Evaluation of ENBREL + MTX vs MTX in moderate to severe RA patients who had failed ≥1 disease-modifying antirheumatic drug (DMARD) other than MTX
The TEMPO Study was a 3-year multicenter, double-blind, randomized, controlled trial (RCT) of 682 patients in Europe, Australia, and Israel with moderate to severe RA (mean disease duration of 6.6 years) who had failed ≥1 DMARD other than MTX. Patients received either ENBREL 25 mg biweekly (BIW) + MTX (n=231), ENBREL 25 mg BIW + placebo (n=223), or placebo + MTX (n=228) over 3 years. Use of concomitant corticosteroids and/or NSAIDs was permitted.1,2,3
*ENBREL + MTX vs MTX (P<0.0001); ENBREL vs MTX (P=0.0034); ENBREL + MTX vs ENBREL (P<0.0001).
†ENBREL + MTX vs MTX (P<0.01); ENBREL vs MTX (P<0.01); ENBREL + MTX vs ENBREL (P<0.01).
‡Major clinical response is achieving an ACR 70 response for a continuous 6-month period.
ENBREL + MTX helps patients feel less joint pain and morning stiffness




ENBREL + MTX can help patients get back to their everyday activities




*HAQ score of ≤0.5 is consistent with the score of the general population.7
ENBREL + MTX can help stop the progression of joint damage


*Per protocol, in order to read the Year 3 data (N=638), the Year 1 (N=648) and Year 2 data (N=622) were reread. Because of known variability in reading of the radiographic images in RA, all radiographs were reread and blinded to patient and time point by the 2 physicians who read the images for the Year 2 report. Thus, the Year 3 scoring of the radiographic images is considered a new reading of the Year 1 and Year 2 time points.
†P<0.01 vs MTX; ‡P<0.01 vs ENBREL.
ENBREL + MTX helps patients achieve clinical remission


ACR, American College of Rheumatology; ACR 20/50/70, American College of Rheumatology (20/50/70) percent response; ACR-N, numeric index of the ACR response; AUC, area under the curve; CI, confidence interval; CRP, C-reactive protein; DAS 28, disease activity score in 28 joints; HAQ, health assessment questionnaire; ITT, intent-to-treat; LOCF, last observation carried forward; mTSS, modified total Sharp score; MTX, methotrexate; NSAIDs, non-steroidal anti-inflammatory drugs; TEMPO, the trial of etanercept and methotrexate with radiographic patient outcomes.
Evaluation of ENBREL + MTX vs MTX in early moderate to severe RA
The COMET study was a 24-month, multicenter, randomized, double-blind, 2-period study of 542 patients with moderately to severely active RA (from ≥3 months’ to ≤2 years’ duration) with mean disease duration of 9 months and mean baseline DAS 28 of 6.5. In Year 1 of the study, patients were randomized to receive once-weekly ENBREL 50 mg + weekly MTX, up to 20 mg/week (n=274); or MTX alone (n=268).9 At Year 2, the original combination group either continued combination therapy (n=108) or received ENBREL monotherapy (n=108); the original MTX monotherapy group either received combination therapy (n=88) or continued MTX monotherapy (n=94).10




*One subject (group 1A) discontinued at final Year 1 visit but received one dose of study drug in Year 2 and was included in the Year 2 population.
| Mean age | 51 Years |
| Percent male/female | 26.7%/73.3% |
| Mean disease duration | 9.0 months |
| Mean HAQ | 1.7 |
| Mean DAS 28 | 6.5 |
| Mean tender joint count | 25 |
| Mean swollen joint count | 17 |
ENBREL + MTX delivers fast symptom improvement


*ENBREL + MTX: n=265, MTX: n=262.
†ENBREL + MTX: n=265, MTX: n=263.
‡ENBREL + MTX demonstrated a mean reduction of 27 mm on a visual pain scale of 100 mm at Week 2 compared to 8 mm for MTX alone.
§ENBREL + MTX: n=262, MTX: n=258.
A patient who responds to ENBREL by Week 12 may see additional improvement at Week 24.1,13


57.4% of partial responders at 12 weeks achieved ACR 50 by 24 weeks13
ENBREL + MTX can help your patients get back to their everyday activities

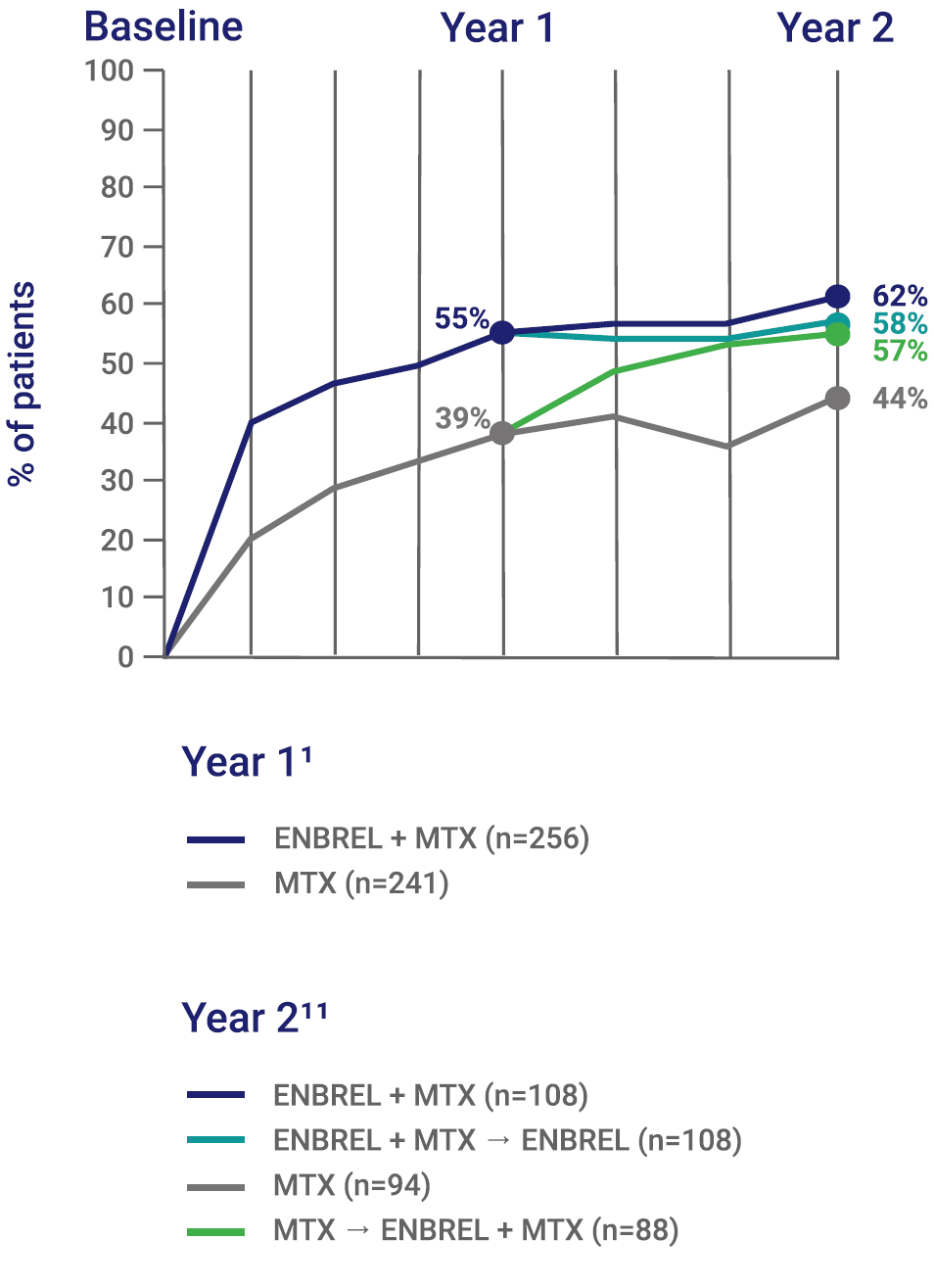
*The data points shown at Year 1 represent results for combined study arms (Group 1A + Group 1B and Group 2A + Group 2B) reported at the end of Year 1 of treatment. For the study populations entering Year 2 of treatment, the percentages of patients who had achieved HAQ ≤0.5 at the Year 1 time point were 57%, 62%, 51%, and 43% in Groups 1A, 1B, 2A, and 2B, respectively.14
†Patients were randomly assigned to 1 of 4 treatment groups (Group 1A, 1B, 2A, or 2B) at the beginning of the study. During Year 1 of the study, Groups 1A and 1B were combined in the ENBREL + MTX treatment arm, and Groups 2A and 2B were combined in the MTX treatment arm. Not all subjects randomized to Year 2 groups were present in the Year 2 efficacy population, due to withdrawals during Year 1. See Study Design for more information about the Year 1 and Year 2 study populations.10
The majority of ENBREL + MTX patients achieved a HAQ score consistent with the general population (HAQ ≤0.5)11,14‡
‡HAQ score of ≤0.5 is consistent with the score of the general population.14
ENBREL + MTX helps stop further progression of joint damage by Year110
*No progression is defined as a change in mTSS ≤0.0 from baseline.12
ENBREL + MTX can help your patients achieve clinical remission


DAS 28 clinical remission was observed in 7 out of 10 patients when treated earlier (post hoc sub-group analysis of very early RA)15
COMET, comparison of methotrexate monotherapy with a combination of methotrexate and etanercept in active, early, moderate to severe rheumatoid arthritis.
Evaluation of etanercept and methotrexate in combination or as monotherapy in subjects with moderate to severe RA
The SEAM-RA Study was a multicenter, randomized, withdrawal, double-blind controlled study that enrolled 371 patients with moderate to severe RA on ENBREL + MTX who had good disease control for 6 months before study entry. The study consisted of a 30-day screening period, a 24-week open-label run-in period, a 48-week double-blind treatment period, and a 30-day safety follow-up period.16 Eligible patients (n=253) who were in SDAI remission (SDAI ≤3.3) were randomized to receive ENBREL + MTX combination therapy (n=51), ENBREL monotherapy (n=101), or MTX monotherapy (n=101).17


*During the double-blind phase, patients with disease-worsening could receive rescue therapy with weekly ENBREL + MTX
(ie, reestablished or continued combination therapy using the same doses received at study enrollment) in an attempt
to recapture remission. Patients were considered to have disease-worsening if they had an increased SDAI score >3.3 and ≤11 on two consecutive visits at least 2 weeks apart, or SDAI >3.3 and ≤11 at any time on three or more separate
visits, or SDAI >11 at any time.
SDAI is a simple calculation and convenient tool for clinical practices to assess remission that’s in addition to DAS 28.† A patient’s SDAI is the sum of the following scores:17,18
†DAS 28 allows for up to 6 swollen joints, and a score of <2.6 meets the criteria for remission. SDAI allows for up to 2 swollen joints, and a score of ≤3.3 meets the criteria for remission.19 DAS 28 requires a value for ESR or CRP and a more complex calculation, for which a calculator may be necessary, while SDAI requires only simple addition of the component values. Lab testing is required.18
| Demographic/ Characteristics |
ENBREL + MTX (n=51) |
ENBREL Monotherapy (n=101) | MTX Monotherapy (n=101) |
|---|---|---|---|
| Mean age in years (SD) | 55.9 (12.6) | 54.8 (12.8) | 56.2 (11.4) |
| % Female | 78.4 | 76.2 | 75.2 |
| Mean disease duration in years (SD) | 10.3 (8.2) | 11.0 (7.4) | 9.7 (8.0) |
| % Rheumatoid factor positive | 68.6 | 63.4 | 58.4 |
| % Anti-CCP positive | 68.6 | 66.3 | 65.3 |
| Mean MTX dose mg/week (SD) | 17.06 (4.99) | 15.97 (4.65) | 16.26 (4.56) |
| Mean SDAI score (SD) | 1.2 (1.2) | 1.3 (1.4) | 1.3 (1.0) |
| Mean HAQ-DI (SE) | 0.28 (0.06) | 0.26 (0.04) | 0.32 (0.04) |
–Patients with disease-worsening had an increased SDAI of >3.3 and ≤11 on two consecutive visits at least 2 weeks apart, or an SDAI of >3.3 and ≤11 at any time on three or more separate visits, or an SDAI of >11 at any time after randomization21
For patients who achieved remission on ENBREL + MTX, ENBREL monotherapy helped more patients maintain SDAI remission than MTX monotherapy16
ENBREL monotherapy helped significantly more patients maintain SDAI remission at Week 48 without disease-worsening compared with MTX monotherapy16


*Non-responder imputation. The primary analysis set included all randomized subjects. The analysis was conducted according to the original randomization assignment regardless of the actual treatment received during the study (as per intent-to-treat principle).
†ENBREL monotherapy vs MTX monotherapy. The risk difference and its P value were estimated from the Chi-squared test with continuity correction.
Patients on ENBREL monotherapy maintained SDAI remission without disease-worsening for a longer time compared to MTX monotherapy at Week 4816
The time to disease-worsening was shorter for patients on MTX monotherapy compared to ENBREL monotherapy16


75% of patients on ENBREL monotherapy who received rescue therapy recaptured SDAI remission by the end of the study16


Of the patients who received rescue therapy in the SEAM-RA Study, most recaptured low disease activity16
92% of patients on ENBREL monotherapy who received rescue therapy recaptured low disease activity by the end of the study16


Based on results of ENBREL's open-label studies, after discontinuation of ENBREL, symptoms of arthritis generally returned within a month. Reintroduction of treatment with ENBREL after discontinuations of up to 18 months resulted in the same magnitudes of response as in patients who received ENBREL without interruption of therapy.1
Anti-CCP, anti-cyclic citrullinated peptide; EOS, end of study; ESR, erythrocyte sedimentation rate; HAQ-DI, Health Assessment Questionnaire Disability Index; QW, every week; SEAM-RA, study of etanercept and methotrexate in combination or as monotherapy in subjects with rheumatoid arthritis; SD, standard deviation; SDAI, simple disease activity index; SE, standard error.
Evaluation of ENBREL and MTX in early moderate to severe RA, including an analysis of MTX discontinuation
The Early RA (ERA) Study was a 1-year, multicenter, randomized, double-blind study of 632 patients with early moderately to severely active RA (≤3 years’ duration) with mean disease duration of 11.2 months. In Year 1 of the study, patients were randomized to receive ENBREL 10 mg BIW (n=208), ENBREL 25 mg BIW (n=207), or MTX (up to 20 mg/week, n=217). At Year 2, patients continued in an open-label treatment period. At Year 3, patients switched to or continued ENBREL 25 mg BIW for an open-label extension (OLE) (n=468). MTX could be continued or started as necessary in the OLE at the investigator's discretion.1,25,26
–There is no concurrent control arm, limiting the estimate of treatment effect
–Data are based only on patients who continued taking ENBREL at each year. Reasons for discontinuation included lack of tolerability, lack of efficacy, and loss to follow-up. Response rates may represent an enriched proportion of patients with continued efficacy and tolerability


*At the end of Year 2, patients switched to or continued on ENBREL 25 mg BIW.


*Patients who received MTX during the first 2 years of the study and who started ENBREL in the OLE.
†Change from baseline of OLE.
‡Patients who received ENBREL during the first 2 years of the study and continued taking ENBREL in the OLE.
§Change from baseline.



**Patients who received MTX during the first 2 years of the study and who started ENBREL in the OLE.
††Patients who received ENBREL during the first 2 years of the study and continued taking ENBREL in the OLE.
‡‡Change from baseline of OLE.
§§Change from baseline.
**Patients who received MTX during the first 2 years of the study and who started ENBREL in the OLE.
††Change from baseline of OLE.
‡‡Patients who received ENBREL during the first 2 years of the study and continued taking ENBREL in the OLE.
§§Change from baseline.
Long-term inhibition of further joint damage through Year 5


No progression is defined as a change in mTSS ≤0.0 from baseline; n=297.
A 10-year post hoc analysis of the ERA Study of moderately to severely active early RA

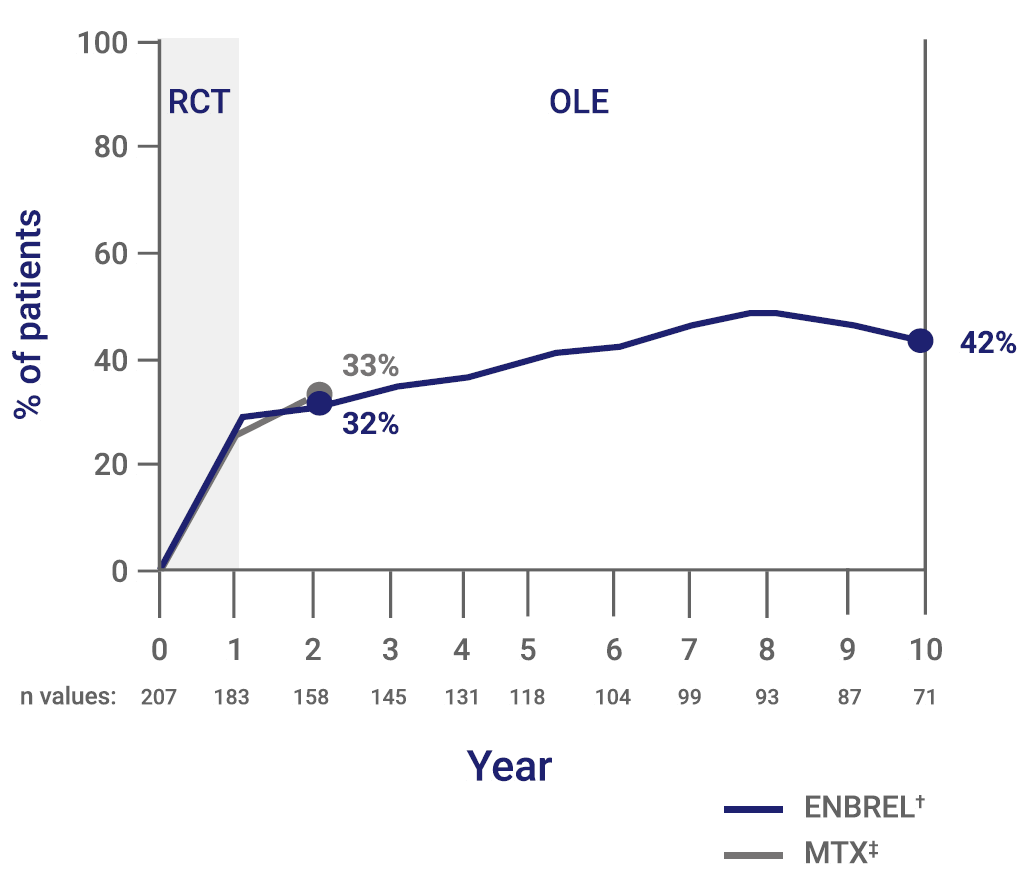
*In this study, a modified DAS, DAS 28, was utilized based on a 28-joint count (28 tender and 28 swollen). DAS 28 clinical remission is defined as DAS 28 <2.6 units.
†Patients were administered ENBREL 25 mg BIW monotherapy for the first 2 years, then continued on ENBREL 25 mg BIW with the option to add MTX at any point during the remainder of the study.
‡Baseline: n=217; Year 1: n=192; Year 2: n=138.
Limitations of DAS 28 post hoc analysis and OLE
Prescription Enbrel® (etanercept) is administered by injection.
IMPORTANT SAFETY INFORMATION AND INDICATIONS
SERIOUS INFECTIONS
Patients treated with ENBREL are at increased risk for developing serious infections that may lead to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids or were predisposed to infection because of their underlying disease. ENBREL should not be initiated in the presence of sepsis, active infections, or allergy to ENBREL or its components. ENBREL should be discontinued if a patient develops a serious infection or sepsis. Reported infections include: 1) Active tuberculosis (TB), including reactivation of latent TB. Patients with TB have frequently presented with disseminated or extrapulmonary disease. Test patients for latent TB before ENBREL use and periodically during therapy. Initiate treatment for latent infection prior to ENBREL use, 2) Invasive fungal infections, including histoplasmosis, coccidioidomycosis, candidiasis, aspergillosis, blastomycosis, and pneumocystosis. Patients with histoplasmosis or other invasive fungal infections may present with disseminated, rather than localized, disease. Antigen and antibody testing for histoplasmosis may be negative in some patients with active infection. Consider empiric antifungal therapy in patients at risk for invasive fungal infections who develop severe systemic illness, and 3) Bacterial, viral, and other infections due to opportunistic pathogens, including Legionella and Listeria.
The risks and benefits of treatment with ENBREL should be carefully considered prior to initiating therapy in patients 1) with chronic or recurrent infection, 2) who have been exposed to TB, 3) who have resided or traveled in areas of endemic TB or endemic mycoses, or 4) with underlying conditions that may predispose them to infections such as advanced or poorly controlled diabetes. Monitor patients closely for the development of signs and symptoms of infection during and after treatment with ENBREL, including the possible development of TB in patients who tested negative for latent TB prior to initiating therapy.
MALIGNANCIES
Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with tumor necrosis factor (TNF) blockers, including ENBREL.
In adult clinical trials of all TNF blockers, more cases of lymphoma were seen compared to control patients. The risk of lymphoma may be up to several-fold higher in RA patients. The role of TNF blocker therapy in the development of malignancies is unknown.
Cases of acute and chronic leukemia have been reported in association with postmarketing TNF blocker use in RA and other indications. The risk of leukemia may be higher in patients with RA (approximately 2-fold) than the general population.
Melanoma and non-melanoma skin cancer (NMSC) have been reported in patients treated with TNF blockers, including ENBREL. Periodic skin examinations should be considered for all patients at increased risk for skin cancer.
Pediatric Patients
In patients who initiated therapy at ≤18 years of age, approximately half of the reported malignancies were lymphomas (Hodgkin's and non-Hodgkin's lymphoma). Other cases included rare malignancies usually associated with immunosuppression and malignancies that are not usually observed in children and adolescents. Most of the patients were receiving concomitant immunosuppressants.
NEUROLOGIC REACTIONS
Treatment with TNF-blocking agents, including ENBREL, has been associated with rare (<0.1%) cases of new onset or exacerbation of central nervous system demyelinating disorders, some presenting with mental status changes and some associated with permanent disability, and with peripheral nervous system demyelinating disorders. Cases of transverse myelitis, optic neuritis, multiple sclerosis, Guillain-Barré syndromes, other peripheral demyelinating neuropathies, and new onset or exacerbation of seizure disorders have been reported in postmarketing experience with ENBREL therapy. Prescribers should exercise caution in considering the use of ENBREL in patients with preexisting or recent-onset central or peripheral nervous system demyelinating disorders.
NEW ONSET OR WORSENING OF HEART FAILURE
Cases of worsening congestive heart failure (CHF) and, rarely, new-onset cases have been reported in patients taking ENBREL. Caution should be used when using ENBREL in patients with CHF. These patients should be carefully monitored.
HEMATOLOGIC REACTIONS
Rare cases of pancytopenia, including aplastic anemia, some fatal, have been reported. The causal relationship to ENBREL therapy remains unclear. Exercise caution when considering ENBREL in patients who have a previous history of significant hematologic abnormalities. Advise patients to seek immediate medical attention if they develop signs or symptoms of blood dyscrasias or infection. Consider discontinuing ENBREL if significant hematologic abnormalities are confirmed.
HEPATITIS B REACTIVATION
Reactivation of hepatitis B has been reported in patients who were previously infected with hepatitis B virus (HBV) and received concomitant TNF-blocking agents, including ENBREL. Most reports occurred in patients also taking immunosuppressive agents, which may contribute to hepatitis B reactivation. Exercise caution when considering ENBREL in these patients.
ALLERGIC REACTIONS
Allergic reactions associated with administration of ENBREL during clinical trials have been reported in <2% of patients. If an anaphylactic reaction or other serious allergic reaction occurs, discontinue administration of ENBREL and initiate appropriate therapy immediately.
IMMUNIZATIONS
Avoid concurrent administration of live vaccines with ENBREL. Patients, if possible, should be brought up to date with all immunizations prior to initiating ENBREL. In patients with exposure to varicella virus, temporarily discontinue ENBREL and consider prophylactic treatment with Varicella Zoster Immune Globulin.
AUTOIMMUNITY
Autoantibodies may develop with ENBREL, and rarely lupus-like syndrome or autoimmune hepatitis may occur. These may resolve upon withdrawal of ENBREL. Stop ENBREL if findings suggestive of lupus-like syndrome or autoimmune hepatitis develop and evaluate the patient.
NOT RECOMMENDED FOR GRANULOMATOSIS WITH POLYANGIITIS PATIENTS ON IMMUNOSUPPRESSANTS
The use of ENBREL in patients with granulomatosis with polyangiitis receiving immunosuppressive agents (eg, cyclophosphamide) is not recommended.
INCREASED MORTALITY IN PATIENTS WITH MODERATE TO SEVERE ALCOHOLIC HEPATITIS
Based on a study of patients treated for alcoholic hepatitis, exercise caution when using ENBREL in patients with moderate to severe alcoholic hepatitis.
ADVERSE REACTIONS
The most commonly reported adverse reactions in RA clinical trials were injection site reaction and infection. In clinical trials of all other adult indications, adverse reactions were similar to those reported in RA clinical trials.
In general, the adverse reactions in pediatric patients were similar in frequency and type as those seen in adult patients. The types of infections reported in pediatric patients were generally mild and consistent with those commonly seen in the general pediatric population.
DRUG INTERACTIONS
The use of ENBREL in patients receiving concurrent cyclophosphamide therapy is not recommended. The risk of serious infection may increase with concomitant use of abatacept therapy. Concurrent therapy with ENBREL and anakinra is not recommended. Hypoglycemia has been reported following initiation of ENBREL therapy in patients receiving medication for diabetes, necessitating a reduction in anti-diabetic medication in some of these patients.
Please see Prescribing Information and Medication Guide.
INDICATIONS
ENBREL is indicated for reducing signs and symptoms, inducing major clinical response, inhibiting the progression of structural damage, and improving physical function in patients with moderately to severely active rheumatoid arthritis. ENBREL can be initiated in combination with methotrexate (MTX) or used alone.
ENBREL is indicated for reducing signs and symptoms, inhibiting the progression of structural damage of active arthritis, and improving physical function in adult patients with psoriatic arthritis. ENBREL can be used with or without MTX.
ENBREL is indicated for the treatment of patients 4 years or older with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy.
ENBREL is indicated for reducing signs and symptoms in patients with active ankylosing spondylitis.
ENBREL is indicated for reducing signs and symptoms of moderately to severely active polyarticular juvenile idiopathic arthritis in patients 2 years of age and older.
ENBREL is indicated for the treatment of active juvenile psoriatic arthritis in pediatric patients 2 years of age and older.
Prescription Enbrel® (etanercept) is administered by injection.
IMPORTANT SAFETY INFORMATION AND INDICATIONS
SERIOUS INFECTIONS
Patients treated with ENBREL are at increased risk for developing serious infections that may lead to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids or were predisposed to infection because of their underlying disease. ENBREL should not be initiated
Patients treated with ENBREL are at increased risk for developing serious infections that may lead to
References: